Towards a unified theory of health—and why natural health matters more than ever
Rob Verkerk, PhD, founder, executive & scientific director
Synthetic peptides, GLP-1 agonists, repurposed drugs, methylene blue, high-dose synthetic vitamins… these are just a few of the trending “wellness” products that are often mixed in with wholesome natural diets, cold and heat therapies, and other biohacks that aim to enhance the quality and—hopefully—the duration of life.
Biohacks don’t work for everyone
But like any hack, none of it works properly unless the hack itself is compatible with the underlying health of the individual, and all the foundational elements of health are adequately catered for. That includes taking into account the status of the body (the ‘terrain’), the diet, lifestyle, psychological and emotional state of the individual, and the way the individual responds to the various stressors to which he or she is exposed.
And over and over again, that’s where it goes wrong. These foundational principles that represent “natural health” are often glossed over, sometimes through lack of time or attention, and sometimes through lack of understanding of what the individual needs to cope with the demands of life.
Where’s your body and mind’s user manual?
Few can be expected to know exactly what their bodies require without specialist support or advice—unfortunately, we don’t get a user manual that explains the intricacies of this extraordinary body, mind and spirit we are gifted with on the journey we call life. This requires a detailed understanding of the ways in which we have, or have not, adapted—during the course of human evolution—to the world around us, and specifically how we cope with today’s heavily anthropogenic environments.
For some, it’s about trial and error. For others, it’s more about muddling along and letting the people in white coats fix problems as and when they occur, with this outsourcing of maintenance and support often becoming especially intense in the latter years of life. For yet others, personal potential is realised as part of a lifelong journey of experience, coupled with input from different specialist practitioners who have themselves spent their lives learning about human bodies and minds, their needs, and how they respond to different interventions and therapies.
The bedrock: natural health
Whichever way you choose to slice the cake of “healthcare”, natural health remains the bedrock. That’s because our evolutionary trajectory has, for the majority of its course, been based on what we today consider to be a “natural” environment: one free from the complex, built environments—and all that goes along with them—that so many now live in; one in which all the chemicals and radiation sources were of natural origin; one in which our ancestors were subjected to bursts of acute stress, whether through pathogens, predators or tribal conflicts, but nonetheless free from the ongoing, often daily chronic stressors that characterise our modern-day anthropogenic environments. Think financial stress, social conflicts, the barrage of negative mainstream news, incessant interactions with mobile phones, ultra-processed foods that push our metabolism to the limit, daily exposure to thousands of new-to-nature chemicals—and the rest.
Against this background, I felt it relevant to rethink some of the fundamentals of natural health, and especially whether it might be possible to postulate a kind of unified theory of health that would apply to all individuals and be relevant to any discipline or modality of medicine.
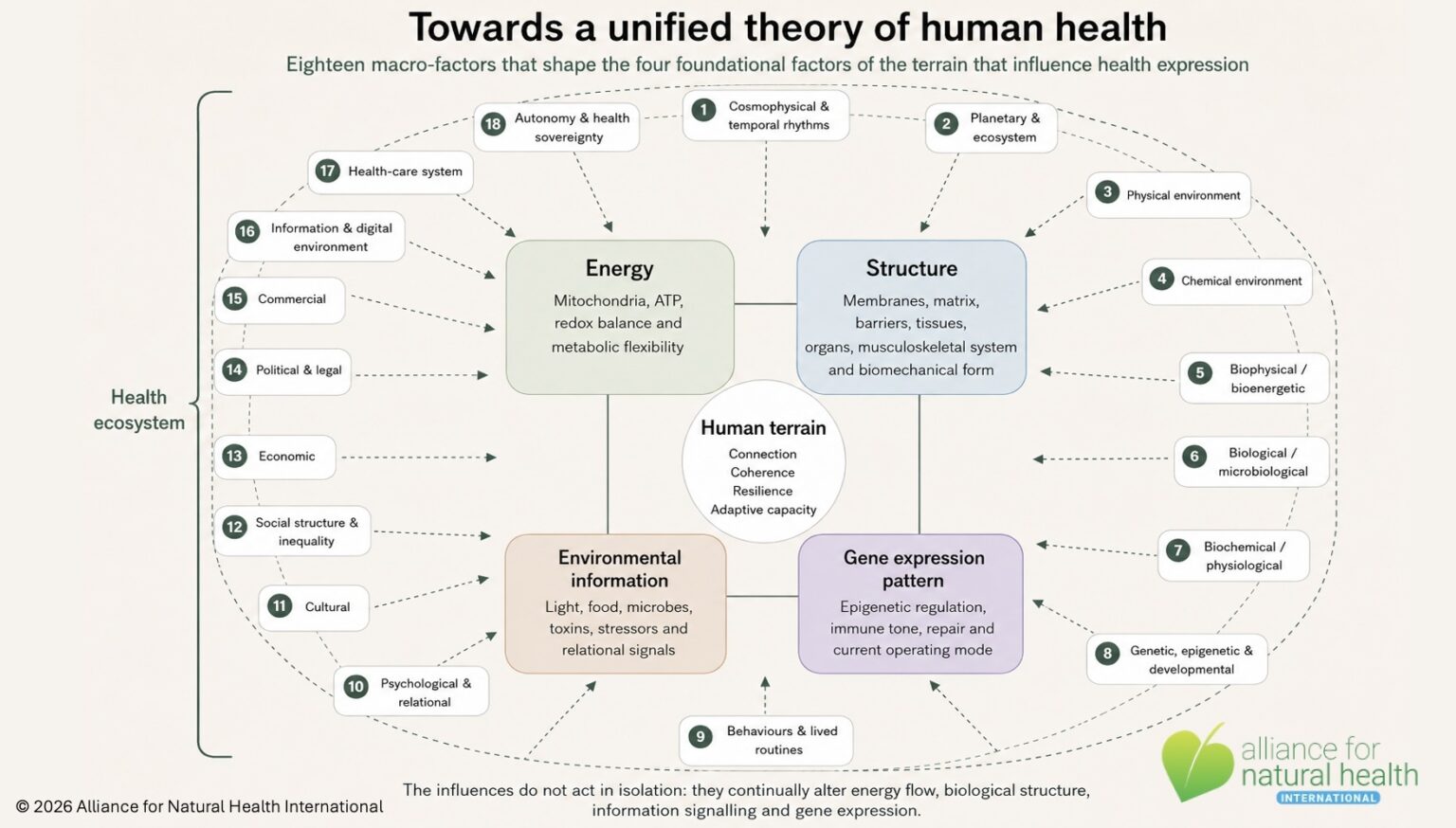
Eighteen macro influences on health
We’ve looked at health influences at ANH in detail before in various practitioner trainings we have run over the years, and my latest incarnation of the summation of published research on health determinants—that we prefer to refer to as influences (for reasons that will be apparent below)— amounts to 18 categories. These are listed below with examples:
- Cosmophysical & temporal rhythms: Photoperiod and circadian/seasonal timing (light–dark cycles), and—more tentatively—solar/geomagnetic disturbances that have been associated with cardiovascular and neurological events.
- Planetary & ecosystem: Climate and weather extremes, biodiversity loss, land use, air/soil/water quality, and ecosystem services fundamental to health.
- Physical environment: Temperature, UV and non-ionising radiation, ambient and indoor air pollution (PM2.5, ozone), noise, light-at-night, green/blue space, built environment and transport.
- Chemical environment: Adaptive stressors (e.g., botanicals), metals, pesticides, endocrine disruptors, volatile organics, pharmaceuticals in water, allergens—endosome/exposome.
- Biophysical / bioenergetic: Light (input/photobiomodulation effects, biophotons), electromagnetic fields (positive and negative influences), vibration/resonance.
- Biological / microbiological: Pathogens; commensal microbiomes; biodiversity exposures (“old friends”); vectors; food webs.
- Biochemical / physiological: Nutrient status, hormones, immune/inflammatory tone, metabolic milieu; homeostatic “hallmarks of health” and age-related hallmarks that modulate disease risk.
- Genetic, epigenetic & developmental (life-course): Inherited variants; prenatal/early-life programming; cumulative and critical-period exposures (exposome focus).
- Behaviours & lived routines: Diet, physical activity, sleep and circadian regularity, substance use, sexual health, oral health, adherence, care-seeking.
- Psychological & relational: Stress, trauma/ACEs, social support, loneliness, mission, purpose and meaning, mental health, spirituality.
- Cultural: Norms, beliefs, language, health literacy, traditional practices; cultural fit of services (Culture & Health Lancet Commission).
- Social structure & inequality: Education, housing, working conditions, discrimination, social capital—core SDOH layers (Dahlgren-Whitehead; WHO CSDH).
- Economic: Income/wealth, employment, market structure, austerity/expansion cycles; affordability of essentials.
- Political & legal: Governance, rights, policy, conflict/peace, regulation of hazards and access to care—“political determinants of health.”
- Commercial: Corporate products and practices (tobacco, alcohol, ultra-processed foods, marketing, lobbying, platform design)—“commercial determinants of health.”
- Information & digital environment: Media, misinformation, advertising architectures, attention economies influencing behaviour and stress. Increasingly, these are treated within commercial/political determinants.
- Health-care system: Access, coverage, quality, continuity, safety, iatrogenesis, cultural acceptability.
- Autonomy and health sovereignty: Locus of control, personal accountability, support, fundamental rights, sound ethical frameworks.
Influences, not determinants
These are macro-categories of influences on health that have been established by various methods that may loosely be referred to as science. In the literature, they are routinely referred to as determinants, but, as alluded to above, we consider it more appropriate to refer to them as influences, as they are not determinate in themselves. That depends on how they act on the ‘terrain’ of the body and mind. Simply knowing about them helps you investigate the ‘health ecosystem’ in which an individual exists, but it tells you nothing about the critical, foundational, universal elements that represent that individual’s terrain, or how they might respond to the influences.
Here, I’m not going to rely on science as such, but rather on personal experience of working most of my life in this field, during the course of which I have digested tens of thousands of research papers, interacted with thousands of different practitioners from a very wide range of modalities, and been privy to hundreds of detailed case studies.
Unified theories — of disease
There have been several attempts to develop a unified theory of disease (not health), including by Professor George Vithoulkas, a leading educator and practitioner in the field of homeopathy, and naturopathic doctor and co-founder of Bastyr University, Joe Pizzorno ND. Vithoulkas relates disease, ultimately, to a form of immune system suppression—an idea that is supported by a considerable body of evidence, even in mainstream medicine. Dr Pizzorno has expounded his thoughts on this subject in an article published in 2020 in the journal for which he is Editor-in-Chief, Integrative Medicine: A Clinician’s Journal. In trying to come to some sort of a unified theory for disease, he argues that there are three things—genetic susceptibilities, toxin overload and nutrient inadequacies—that are always present and can be regarded as primary “causes of disease.” Causes (to which Dr Pizzorno refers) and determinants or influences (that I listed above) are of course not the same thing. Causation in itself isn’t as straightforward or linear as one might expect. As the causal pie model originally proposed by Rothman in 1976 demonstrates, causes may be component, sufficient or necessary (see explanation on CDC archived website).
For me, while I am a huge fan of both Prof Vithoulkas and Dr Pizzorno, and while both have distilled the causes of disease to no more than three factors, I am concerned that these theories still conflate triggers, drivers and mediators of disease with causes. For example, what suppresses the immune system? Isn’t immune suppression a consequence of something that provides the conditions that allow disease to manifest? Where does the impact of abuse or trauma (be it physical, chemical or emotional) fit in? What about psychosocial stress derived from difficult familial or work relationships? Or lacking sufficient meaning in life? Or being too sedentary? And perhaps the biggest one of all: ageing. It is increasingly clear that the factor most consistently associated with chronic disease is ageing. But is it a cause, or a driver? As the paper cited in the previous hyperlink proposes, it’s probably better considered a driver than a cause. Our own lived experience supports this: we all know, or are aware of, some people who can live to a great age with very little evidence of any chronic disease.
Towards a unified theory of health
Perhaps the reason we still seem so far from developing consensus on any kind of unified theory is that we—as a medical and scientific community—are all too preoccupied by disease more than we are by health. Disease represents the downstream consequences of the (often many) things that upset the balance that gives us good health and resilience, in this exquisitely complex system we call a human being. The medical world—in my view—has spent far too long focusing on the wrong side of the health/disease coin. It also sometimes fails to address existing knowledge that helps us understand life—both human and non-human—as we know it. This was a subject of a 2025 feature that I authored, entitled What is life? Energy, information, fields—and purpose without mysticism. The article focuses on 8 discrete characteristics that are consistently associated with life.
With this in mind, in the present article, I propose an alternative view on a unified theory of health, not disease. It’s nothing more than a theory, and it’s one that comes—as I mentioned above—from my own understanding and experience, as a systems-based ecologist, toxicologist, health and environmental scientist.
The concept of disease causation emerged originally from a deterministic, Pasteurian perspective where, to put it simplistically, A + B under condition C yields disease. This might be where A is the individual (or host), B is a pathogen and C is the environment. The trouble is that we know most common diseases are much more complex than this. Even when one looks at the epidemiology of infectious diseases, we know many people can be exposed to a given pathogen and not express disease (i.e., they are asymptomatic). Rare diseases that have genetic origins, such as inborn errors of metabolism, may be exceptions in which a deterministic model fits the bill perfectly.
Deterministic or probabilistic?
When we look at the sheer burden of chronic and degenerative diseases that are now threatening to collapse health systems around the world, it’s very difficult indeed to identify consistent causative agents or factors. What we see instead is a tendency for certain constellations of factors to be associated with specific conditions or diseases. This points towards a probabilistic model, rather than a deterministic one, being the general rule of thumb. Mark Parascandola from the Division of Cancer Control and Population Sciences at the National Cancer Institute (USA) explained in his 2011 paper that epidemiologists are still haunted by the debate over whether probabilistic or deterministic models are more important. The reality is that the science of epidemiology, while becoming ever more established as a discrete and influential discipline, remains approximate. That’s not just because of the limitations of the methods used; it’s often because the data required to make accurate deterministic or probabilistic assessments are frequently lacking.
As I have intimated above, I lean strongly towards the probabilistic side of this hot debate. What often seems to occur—to use the generalised model above—is that, in the presence of health influences A, B, C, D and E, when the underlying terrain of the individual can be described by factors V, W, X, Y and Z, there is a reproducibly enhanced risk of a chronic or degenerative disease compared with an individual in whom these influence and terrain factors are absent. The influencing factors, for example, might be: A = poor lifelong diet, B = sedentary behaviour, C = exposure to chronic stress, D = toxic overload and E = low socioeconomic status. The underlying conditions of the terrain might be: V = older age (over 60 years), W = persistent low-grade inflammation, X = immune dysregulation, Y = mitochondrial insufficiency and Z = unfavourable epigenetic pattern of expression.
Such a model can’t be deterministic because these won’t be the only health influences, nor will the terrain factors be the only ones that make the individual’s terrain susceptible. Yes, the overall ‘health ecosystem’ that leads a body from a place of homeodynamic balance to one of imbalance that manifests in one or more pathologies is much more complex than that!
Proposing ANH’s unified theory of health
As I explained above, there is a field of some 18 major sources of influence on the health of an individual. But this is where I attempt to distil what happens at, and within, the level of the individual to just four factors. Okay, I accept failure compared with Prof Vithoulkas’ single factor and Dr Pizzorno’s three factors; but they were focusing on disease, not health. The purpose is to offer a model that is universally applicable to all humans, irrespective of ethnicity or culture, relevant to all environments, and all medical modalities.
The unified theory of health that I propose, in its basic form, is explained in the following diagram:
The model—assuming its value—confirms why mainstream medicine, with its strong focus on drug-based interventions and surgery, does so little to prevent chronic and degenerative diseases. It works in a different space. It is neither designed nor equipped to modify or improve the four underlying factors intrinsic to the terrain, nor is it set up to help identify and modify the multiple negative influences on the human terrain.
More importantly, the model may help both health professionals and their patients or clients identify and address critical aspects of health that are fundamental to resilience. This may often be about better understanding and resolving evolutionary mismatches that will otherwise lead to to the common soil of disease. This common soil, as I explain in a short article recently published in Open Access Government, comprises four interrelated elements: (1) persistent, low-grade inflammation where the body is stuck in smouldering inflammation that never quite switches off; (2) its cells are subjected to oxidative stress which leads to premature aging, damage to membranes and DNA; (3) immune dysregulation where the immune system becomes confused, often overreactive and sometimes suppressed, and; (4) mitochondrial insufficiency, where the tiny power‑plants in our cells—the mitochondria—start running inefficiently, producing less energy than needed as well as more ‘exhaust’ byproducts that apply further stress to the body.
Flipping back to health from the disease side of the coin, in short, where there is abundant biochemical energy in the system, coherent bioelectrical and electromagnetic fields, cellular and other structures that maintain their integrity, appropriate dietary inputs and signalling from environmental information, along with patterns of gene expression that promote health, disease will struggle to manifest.
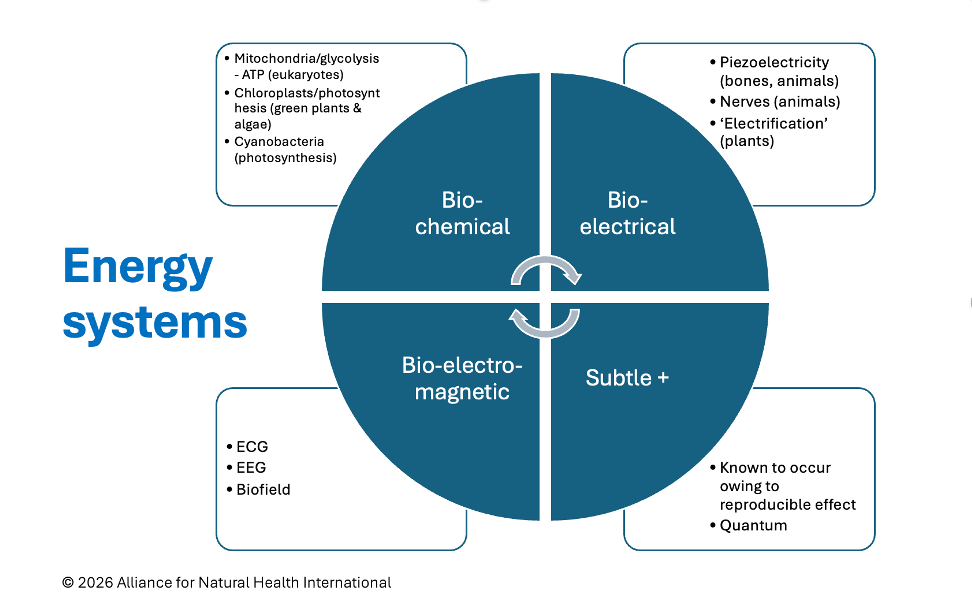
Different forms of energy associated with human beings
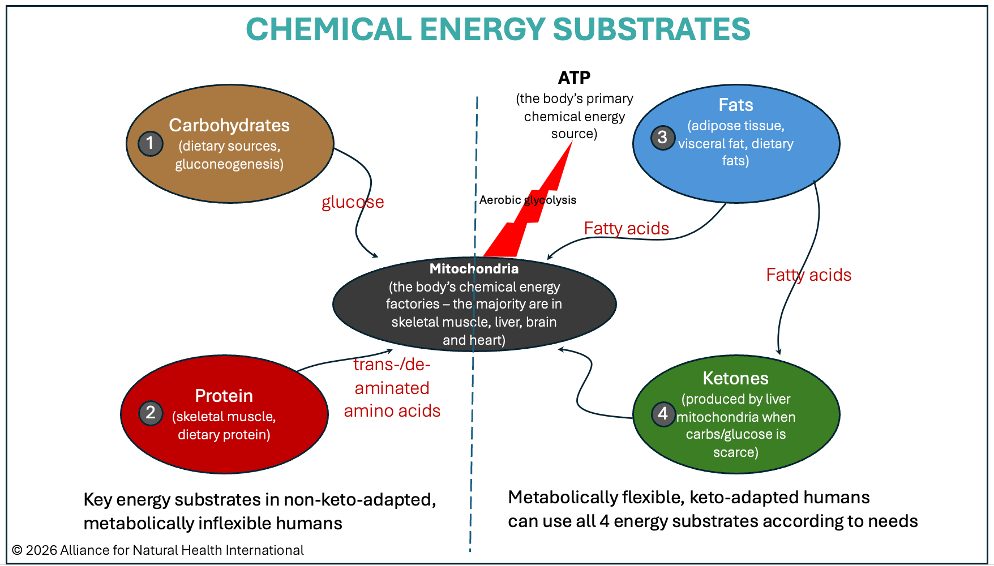
Substrates used by human beings to create biochemical energy (adenosine triphosphate, ATP)
The perspective from this unified theory of health may help us to focus on the things we often ignore. It turns out, the things that really matter are the very things we tend to ignore. They seem overly simple, they’re hard to profit from, they require effort to implement, and they’re not easily delivered by health systems. Take sitting, for example. Sitting is the new smoking, but sitting for hours each day and being sedentary feeds directly into the 4-factor common soil. What we eat, when we eat, and how we eat are also incredibly important. Public health messaging tells us to eat a bit more fruit and veg, less salt, less sugar, less fat, and less ultra-processed foods, but not all of this governmental advice is based on good science. And none of it addresses the fact huge numbers are still consuming gluten-containing grains that impact the tight-junctions in their gut contributing to permeability which can be a key factor into persistent low-grade inflammation. The fruits and vegetables we eat simply don’t deliver the same punch of antioxidants and cancer-fighting compounds as those our grandparents consumed, especially if we consume many as ready-made meals. Modern eating habits including regular snacking pushes the body into a pro-inflammatory state so the gut simply doesn’t have a chance to turn-off its immune system-induced inflammatory fire which it can only do when left in a fasted state say for 16-hours during each 24-hour cycle.
Concluding remarks
This way of looking at health is not intended to replace the important work done by those who have helped map the wider determinants of health—from Dahlgren and Whitehead’s now famous “rainbow model,” to Sir Michael Marmot and the WHO Commission on Social Determinants of Health, and more recent work on the commercial determinants of health.
These frameworks have been vital in showing us that health is never just a matter of personal choice, nor simply the downstream product of genes, biochemistry or medical care. It is shaped continuously by the environments, systems, relationships, policies, and cultural and commercial forces in which we live.
But from the standpoint of the individual human being—the living, breathing, adapting organism—these influences must still be translated through the body’s core operating systems. They must alter energy production, physical and biological structure, the flow of environmental information, or the patterns of gene expression that determine whether the body is in a state of repair, resilience and coherence (organisation or reorganisation), or in a state of defence, degeneration and eventual disease (entropy). This includes the ongoing metabolic interplay between anabolism and catabolism described by Laurent Schwartz and colleagues in their 2021 article, Metabolic Shifts as the Hallmark of Most Common Diseases: The Quest for the Underlying Unity.
Natural health matters now more than ever because it is the discipline, philosophy and practice that best understands this terrain. It asks not merely what can suppress a symptom, override a pathway, or extend a lifespan on paper, but what supports the conditions through which a human being can remain adaptive, connected, functional, purposeful—and truly alive, in a state in which human flourishing is the norm rather than the exception.
Source of information – Alliance for Natural Health (ANH) https://anhinternational.org/
This article was published with the permission of ANH
Photo credit – pixabay.com